AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2693-4779/026
1* Outcomes Research Consortium, University of Texas Southwestern.
2 University of Louisville, Louisville, KY.
*Corresponding Author: Anupama Wadhwa, University of California, San Diego. CA, USA.
Citation: A Wadhwa, Sunitha K Kandadai, S Chhabra, Alexander B, U Schmidt, H M. Koenig. (2021) Intraoperative Intravenous Methadone and Ketamine Combination versus Intravenous Morphine and Ketamine Combination for Post-Operative Analgesia in Patients Undergoing Lower Extremity Fracture Surgery. Clinical Research and Clinical Trials. 3(4); DOI:10.31579/2693-4779/026
Copyright: © 2021 Anupama Wadhwa, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 February 2021 | Accepted: 02 April 2021 | Published: 10 May 2021
Keywords: intravenous; methadone; ketamine; morphine; lower extremity fracture; pain control
Background: Pain management for lower extremity fracture surgeries can be challenging. The purpose of this study is to determine whether the use of ketamine and methadone are more effective than ketamine and morphine to reduce postoperative pain and morphine requirements in patients undergoing lower extremity fracture surgery.
Materials and Methods: Seventy-five patients 18-65 years of age, ASA class I-III, were enrolled in this study, which scheduled for elective lower extremity orthopedic surgery involving fracture of femur or tibia were recruited for the study. Thirty-eight randomized to the Methadone group and 37 randomized into the Morphine group.
Participants were randomized to either one of the two groups: methadone (2ug/kg fentanyl, 0.2 mg/kg ketamine and 0.2 mg/kg methadone IV) versus control (2 ug/kg fentanyl, 0.2mg/kg ketamine and 0.2 mg/kg morphine IV). The primary outcome was total morphine equivalent (MEQ) during the first 24 and 48 hours after surgery. Secondary outcomes included postoperative pain scores in PACU, at 24 and 48 hours, as well as postoperative nausea and vomiting (PONV).
Results: There was no difference in intraoperative consumption of fentanyl between the Methadone group 360mcg and Morphine group 344mcg. In the first 24 hours postoperatively, the Methadone group consumed less MEQ compared with the Morphine group (36.1 mg vs 54.8 mg, p=0.0072), showed lower pain scores than the Morphine group (p=0.0146), and experienced more nausea and vomiting than the Morphine group. There were no differences in sedation in both groups.
Conclusion: The intraoperative use of intravenous methadone significantly reduced post-operative opioid requirement in patients undergoing lower extremity fracture surgery. The results also demonstrated the methadone group had a higher rate of PONV.
Postoperative pain resulting from lower extremity fracture surgeries especially tibia fractures can be excruciating, sometimes lasting for several days after hospital discharge. Pain management in these patients can be a challenge to both anesthesia providers and orthopedic surgeons. Undertreated moderate-to-severe post-surgical pain can predispose patients to persistent pathologic or chronic pain states and cause significant morbidity and disability [1-4].
Intravenous morphine is the traditional opioid used for perioperative pain control in surgical patients but by itself it is not very effective in controlling movement pain. Therefore, it is often combined with NMDA antagonists to treat movement related acute pain that may have beneficial effects on chronic postoperative pain [5-9].
Methadone is a synthetic opioid with mu receptor agonist like morphine and has NMDA receptor antagonist activity like ketamine [11-13] Methadone is attractive as a peri-operative analgesic due to its rapid onset of action, long elimination half-life, which provides prolonged analgesia to treat persistent pain, and its NMDA antagonism, which treats neuropathic component of pain and may prevent opioid tolerance and opioid induced hyperalgesia. Methadone has been successfully and safely used in patients undergoing spine surgery, laparoscopic surgery and cardiac surgery, resulting in improved postoperative pain control [14-15]. In addition, methadone has been shown to provide superior pain control than morphine in patients undergoing upper abdominal surgery, total hip arthroplasty and cesarean delivery [16, 17] Lower extremity surgery can have moderate to severe pain, needing large doses of opioids and patients often become tolerant to these opioids. Surgeons prefer no regional anesthesia for lower extremity surgery due to risk of compartment syndrome because of the tight muscle compartments in thigh and calf [18].
We performed this randomized controlled study to test the hypothesis that ketamine and methadone are more effective than ketamine and morphine to reduce postoperative pain and postoperative morphine requirements.
This study was performed at the University of Louisville Hospital. The University of Louisville Human Studies Committee approved the protocol, and all participants gave written informed consent before participating in the study. This trial was registered with Clinicaltrials.gov with identifier NCT00892606.
The study included consecutive patients with ages between 18-65 years with ASA class I-III, who presented for elective lower extremity orthopedic surgery involving fracture of long bones (femur or tibia) and expected to last more than one hour. Patients with any known contraindications to methadone or morphine were excluded. This included hypothyroidism, Addison's disease, prostatic hypertrophy, known hepatic or renal dysfunction or urethral stricture. Pregnant patients, patients with BMI more than 35 or known respiratory or cardiovascular function were also excluded. Patients taking drugs that induce or inhibit p450 enzyme systems or who needed opioids in the two weeks before surgery were excluded. A preoperative EKG was done on all patients to assess the baseline QTc and if prolonged (>450 msec), they were excluded from the study.
Statistics: A power analysis was performed -to measure a 40% reduction of morphine consumption in the first 48 hours postoperatively in the methadone group, a 38 patients in each group were needed to achieve 90% power at a significance level of 0.05. Summary statistics on the demographic and outcome data were expressed as means +/- SD for continuous values and percentage for the categorical values. A two-way ANOVA using repeated measures was used to analyze the data and adjusted Tukey's test. All analyses were performed using SAS version 9.3 and with a statistical significance of 0.05.
The randomization codes were computer-generated and stored in opaque envelopes until opened. The unblinded investigator opened the randomization envelope to determine patient group assignment after informed consent was obtained. The patients were randomized to one of two groups: Patients in methadone group received 2 µg/kg fentanyl, 0.2 mg/kg ketamine and 0.2 mg/kg of methadone IV and patients in the control group received 0.2 mg/kg ketamine, 2 µg/kg fentanyl and 0.2 mg/kg of morphine IV with induction of general anesthesia. Methadone and morphine were administered after the patient was intubated successfully as confirmed by end tidal carbon dioxide.
Patients received 1- 4 mg midazolam before being transferred to the operating room, at the discretion of the anesthesia care team not involved in the study. All patients were monitored with standard ASA monitors. The anesthesia provider (resident/certified registered nurse anesthetist/attending) and the research fellow who followed the patient (2nd investigator) in the PACU were blinded to the study drug given to the patient.
Patients were anesthetized with propofol 2 mg/kg or etomidate 0.2 mg/kg, 0.2 mg/kg of ketamine and rocuronium 1 mg/kg, per the anesthesia provider. After intubation, the study drug (0.2 mg/kg of morphine or methadone diluted to 10cc) was administered by the blinded anesthesia provider to the patient. Anesthesia was maintained with oxygen, air and an inhalational agent of anesthesiologist’s choice to a targeted BIS between 40 and 60. Additional analgesia was provided with fentanyl in 50 µg increments at the discretion of the anesthesiologist. At the end of surgery, the neuromuscular block was reversed and fentanyl was titrated to maintain a spontaneous respiratory rate of 12-15 breaths per minute and 8-10 ml/Kg tidal volumes to meet extubation criteria. The intraoperative use of narcotics, sedatives and anesthetic drugs were recorded. The type of surgery, duration of surgery and use of additional analgesics and antiemetics were noted.
An investigator blinded to randomization tracked the patients in the PACU. In the recovery room, morphine was given in 2-4 mg increments intravenously up to a total of 20 mg, if they reported a verbal rating pain scale (VRS) more than 4. If the patients continued to report pain (VRS > 4) after 20 mg morphine was given, intravenous hydromorphone was given in 0.5 mg dose every 15 minutes (maximum dose 4 mg) until the patient had adequate analgesia (VRS < 4). Patients received morphine patient-controlled analgesia (PCA) for pain relief as the primary analgesic. The PCA was adjusted at 1 mg morphine with a 6-minute interval lockout and 10 mg/ hour maximum dose. Acetaminophen and oxycodone combination 500 mg/5 mg were prescribed on the floor as needed, to maintain VRS < 4.
In the PACU, vital signs including respiratory rate, heart rate, non-invasive blood pressure (NIBP), sedation score and oxygen saturation were recorded every 15 minutes. VRS for pain were obtained from the patient every 15 minutes until the patient was discharged to the floor. The investigator also recorded the sedation scores every 15 minutes using the following scale until patient was discharged to the floor:
0-Patient is fully alert
1-Patient has intermittent sedation
2-Patient sedated but responsive to verbal stimuli
3-Patient unresponsive to verbal stimuli
Patients were seen at 8 am and 4 pm on postoperative day one and two and at 8 am on the morning of postoperative day three after surgery, if they were still in the hospital. The initial dose of rescue analgesics and time it was given and was recorded. VRS at rest and on movement was recorded, when the patients were seen. Morphine equivalent required during the first 24 and 48 hours after surgery, as well as incidence and severity of postoperative nausea and vomiting (PONV) was recorded.
Our primary outcome was total morphine equivalent (MEQ) consumption during the first 48 hours after surgery. The secondary outcomes were pain scores in PACU, the worst pain scores in the first 24 hours and 48 hours and time to initial dose of rescue analgesic. Respiratory rate to detect respiratory depression and PONV were recorded.
Seventy five patients were included in this randomized study with 38 patients receiving Methadone with ketamine and 37 receiving Morphine with ketamine. One patient in the methadone/ketamine incorrectly received morphine (This patient should excluded from statistical analysis); however, this patient is included in the group to which they were randomized, for intent to treat analysis. All patients are available for follow-up during recovery and the first 24 hours periods; however, in the second 24 hours period, 4 and 5 patients were lost to follow-up in the Morphine and Methadone groups, respectively.
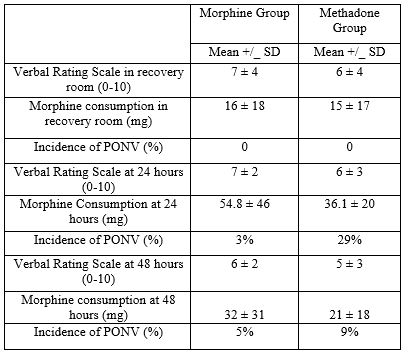
Demographic data are presented in Table 1.The average age and BMI were comparable for the Morphine and Methadone groups. There were more males in both the Methadone and the morphine groups. The intraoperative fentanyl use was 344 mg for the morphine group and 360 mg for the methadone group. (Table 1)

Peri-Induction consumption of sedatives and analgesics was not different between the Morphine and the Methadone groups. (Table 2).

Post-operative morphine equivalents consumption differed significantly during the first 24 post-operative hours (p=0.0031); however, there were no detectable differences in VRS during recovery or the post-operative period. The Methadone group consumed less morphine equivalents (MEQ) than the Morphine group (36.1 mg vs 54.8 mg) at 24 hours (Table 3).
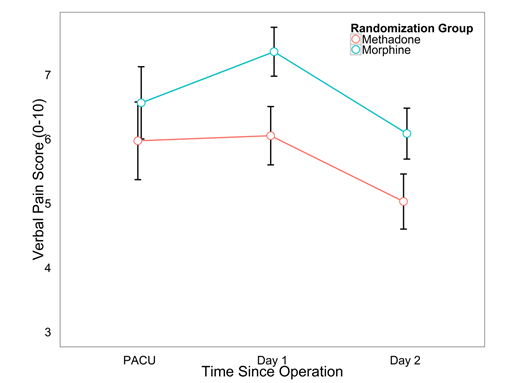
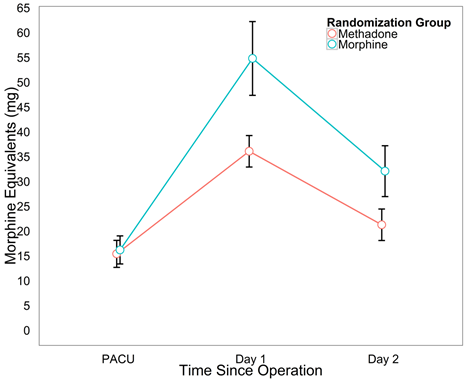
For each group and by time period, Figures 1 and 2 show the average morphine equivalents consumed and verbal rating sale (0-10), respectively. Overall, the Morphine group consumed more morphine equivalents (p = 0.0072) and showed higher pain scores (p = 0.0146) compared to the Methadone group. Additionally, the figures show a relationship between increased morphine equivalent consumption and worse pain scores.
In the first 24 post-operative hours, the Methadone group showed higher rates of nausea/vomiting than the following 24-hour period (29.0% vs. 9.1%, p=0.004),Table 3). The Morphine group had a lower incidence of postoperative nausea and vomiting in the first 24 hours after surgery but the incidence of nausea/vomiting doubled from 24 to 48 hours (2.6% vs 5.4%,Table 3).
Patients’ vital signs were also measured in recovery and compared. No differences were found in MAP_Q30 (98.1 vs 95.8), MAP_Q60 (96.7 vs. 98.1), SPO2_Q30 (97.9 vs. 97.7), SPO2_Q60 (97.9 vs. 97.9) for the Methadone and Morphine groups, respectively. Sedation levels were tracked at 30 and 60 minutes in recovery and during the first and second 24-hour post-operative periods. At all time periods, there were no differences in sedation; however, levels of sedation decreased significantly at each visit (p < 0.0001).
The main finding of this study was that the addition of intraoperative methadone to ketamine significantly decreased postoperative opioid requirements compared to morphine combined with ketamine.
Ketamine, a NMDA antagonist, binds non-competitively to phencyclidine binding site of NMDA receptor in low analgesic or sub anesthetic doses, acted synergistically with opioids and produces better quality of analgesia and opioid sparing effect in a variety of painful surgical procedures [8, 14]. Given the severe and difficult to control pain observed in lower extremity fracture surgery in the immediate postoperative period, it is important to investigate effective combinations and regimens that would benefit patients without use of regional anesthesia. Regional anesthesia is relatively contraindicated in these patients because of the possibility of compartment syndrome that can go unrecognized.
Methadone is a synthetic opioid with mu receptor agonist an receptor antagonist activity. It has long been associated with the treatment of addiction to heroin. There has been a resurgence of interest in the use of methadone as a perioperative analgesic agent within the last decade. In addition, it prevents reuptake of serotonin and norepinephrine. It is commercially available as a racemic mixture of a D- and L-isomer compounds, each optical isomer has distinct opioid receptor affinity but the L –isomer is more physiologically active [19]. Methadone has a variable bioavailability of 40-99 % after oral administration that can potentially lead to serious side effect [19, 20]. It has an oral to parenteral potency ratio of 1: 2 with a long plasma half-life, approximately 24-48 hours (but has a wide inter-individual variability of 13-50 hours), when larger doses are given (≥ 20 mg). The onset of action of intravenous methadone is rapid and comparable to the onset of action of fentanyl and sufentanil [15]. The duration of analgesic effect approximates the half-life of the drug (24-48 hours). It is lipid soluble and has high binding to plasma proteins [16]. These properties of intravenous methadone make it an attractive peri-operative analgesic due to its rapid onset of action, long elimination half-life and its NMDA antagonism, which treats movement pain and prevents opioid tolerance and hyperalgesia. Methadone is primarily eliminated by metabolism and has no active metabolites, unlike morphine and other opioids. A single dose does not cause accumulation. However, one important issue which can arise during methadone treatment is related to its high variability in metabolism [17].The CYP3A4 enzyme found mainly in the liver and in the intestines, metabolizes methadone. The 1-30 fold variability in methadone metabolism is attributed to the variability of expression of this enzyme. Because methadone is mainly metabolized in the liver, it is subject to changes in metabolism by drugs that induce or inhibit the CYP3A4 enzyme such as antifungal and antiretroviral drugs, barbiturates, dexamethasone, and macrolide antibiotics [17]. This can lead to potentially higher levels than expected.
Methadone is proven to be efficacious as a perioperative analgesic in a variety of surgeries like laparoscopic, complex spine and cardiac surgery- all with high degree of pain [19,20, 21]. (Gourlay et al., 1982)[22]. they also had significantly less nausea and vomiting compared with morphine group [23]. The results of our study are comparable to studies with published data in terms of pain relief but our patients had a higher rate of PONV [24].
Patients with lower extremity surgery benefit from having a long acting opioid like methadone, because of severe and prolonged pain associated with these procedures and inability to provide regional anesthesia for them. The higher incidence of postoperative nausea and vomiting may limit its use, but more studies may needed to be performed to determine effects of using supra prophylaxis of anti-emetic therapy with the use of methadone. In our study, we used a standard anti-emetic prophylaxis that was proportionate to the risk profile of the patient. None of our patients had obstructive sleep apnea and we cannot comment on the effects of methadone in patients with obstructive sleep apnea. In our study, we did not observe an increased risk of respiratory depression for the 24-48 hours period.
Although the patients self-administered PCA to reach a VRS score of 6-7, which is higher pain score than acceptable, patients needed less morphine to reach that pain score. We believe that when patients are in extreme pain, they may not aim for VRS scores of less than 4 and they create self-expectations of higher pain scores.
Our study has several limitations that decrease the generalizability of its results. This was single center study in an academic tertiary care center. It is unclear whether the results can be generalized to other settings. We compared methadone and ketamine to methadone and morphine. It is unknown whether the results would be the same for other narcotics and whether the addition of ketamine altered the outcome. We did not follow the long-term outcomes at 30 and 60 days to see if there was any difference in the incidence of chronic pain.
Patients benefit from receiving longer acting opioids like methadone in combination with ketamine when compared with morphine and ketamine. They need substantially less morphine equivalent to reach and maintain the same verbal rating score analogue scale on pain scores.
No potential conflict of interest relevant to this manuscript was reported.
No funding was received.
Our special thanks to Dr. Greg Murphy for providing expert opinion on the manuscript.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
